Date: 07-07-2022
Written by: Dominic Denison-Pender, Business Development Director at The New Life Centre.
Medically Reviews by: Dr Amal Beaini MBChB FRCPsych (Medical Director and Consultant Psychiatrist at The New Life Centre)
1. Overview of Drugs and Other Treatments Preventing Relapse
Probably more patients experience relapse post treatment than go straight into sustained abstinence. Sadly this remains the commonly held expectation, especially as far as opioids are concerned. If “prevention” is taken to be an absolute term, then it is probably not the right word to use in relation to post addiction relapse treatment. Even the most successful addiction treatment, the BONDS Protocol as practiced at The New Life Centre (NCL), is prepared for some patients to relapse, but expects BONDS Protocol treatment that these to be the exceptions rather than the norm. “Relapse reduction” possibly better describes the expectations of most addiction treatment facilities. However the addiction treatment industry (including NCL) tends to talk about “relapse prevention” so we will retain that terminology from here on.
In brief, naltrexone is the only medication specifically used to aid relapse prevention, but at present it is taken by only a very small proportion of patients in addiction treatment. Before looking more closely at the properties and use of naltrexone, it is worth placing such use in the context of what is happening in the addiction treatment sector as a whole.
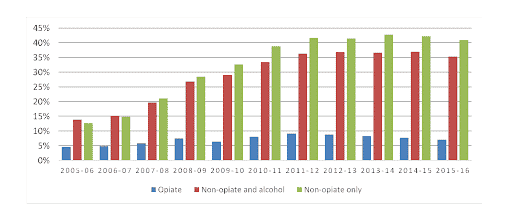
Of course it is the aspiration of all addiction treatments to release patients completely from their patientive dependencies, but the sad truth is that success rates are poor, and dramatically so for opioids. This is clearly illustrated by the following chart extracted from he 2017 Public Health England report entitled “An evidence review of the outcomes that can be expected from drug misuse treatment in England”:
Trend in proportion of individuals (aged 18 and over) successfully completing treatment by substance

Since the latest year covered by the above chart the situation has become even worse. Perhaps the most depressing aspect of opioid addiction in particular is that it tends to go on and on and on. This sorry situation is nowhere better summarised than in the excellent 2020/21 Independent Review undertaken by Dame Carol Black:
- Half of heroin users in treatment have been using the drug for 21 years or more, with 1 in 7 using for over 30 years
- The proportion using for longer periods is increasing year on year as fewer recently initiated users of heroin commence treatment
- Thirty per cent of opiate users have been in treatment for over five years continuously with nearly 1 in 6 in treatment for over 10 years
- People using heroin and those in treatment continuously for longer periods are significantly less likely to complete treatment successfully
- While illicit heroin use falls substantially during treatment, there are around 1 in 4 people still using irrespective of length of time in treatment.
Naltrexone can only be administered as a relapse prevention drug once the patient is totally “clean” and “challenge” tests have proven that this is the case. This means that for most addictions treatment patients naltrexone is simply not an option within the scope of the initial treatment programme.
So let’s look at the treatment programmes and therapies that are most commonly used in the UK.
Easily the most commonly used therapy across the whole range of addictions is the 12-Step programme, the origins of which dated back to the founding of Alcoholics Anonymous in Ohio in 1935. 12-Step is not a scientific or medical programme. It is rather spiritual (involving submission to “a higher power” of the patient’s choosing) and behavioural. It forms the basis of the meetings of mutual support groups such as Alcoholics Anonymous (AA), Drugs Patients Anonymous (DAA) and Narcotics Anonymous (UKNA in the UK). Since none of these groups keep member records as a matter of policy, it is impossible to know how successful the approach is for each type of addiction. 12-Step is also used in many other treatment centres, including several of the best known private residential clinics in the UK. Since detox does not specifically form part of the 12-Step programme, it cannot in itself be seen as a route to naltrexone based relapse prevention treatment.
As far as opioid addiction treatment is concerned, the most commonly used medicated approach is Opiate Substitute Treatment (OST). OST does not in the first instance aim to bring the patient to a state of abstinence that would allow naltrexone based relapse prevention treatment to be initiated. OST aims to transfer the patient from illegal or prescription opiates to less harmful opioid substitutes such as methadone or buprenorphine. Of course the ultimate hope is that the patient will become fully abstinent, but the quotes from the Dame Carol Black Report shown above illustrate what a long drawn our process that tends to be. OST is the most common approach to outpatient opioid addiction treatment.
The use of medication assisted detoxes (MAT) is confined mainly to the residential clinic sector. Naltrexone is one of the medications used to ease the withdrawal symptoms. Such detoxes aim for abstinence rather than a transfer to OST so in principle should enable naltrexone based relapse prevention treatment to be initiated prior to discharge. No data are available on the proportion of patients taking such naltrexone treatment. The detox process and subsequent inpatient rehabilitation therapies (including 12-Step is several such clinics) take considerably longer than is the case at The New Life Centre. It is likely that naltrexone relapse prevention treatment is considered merely as an option. Most is tablet based.
2. Which Drugs are given most commonly to prevent relapse?
Naltrexone is the only drug given as a specific relapse prevention treatment. Naltrexone taken orally is a long-acting, opioid antagonist with high affinity to mu-opioid receptors. A daily dose of naltrexone (50 mg) will block the pharmacologic effects of 25 mg IV heroin for as long as 24 hours, and increasing the dose extends its duration of action to 48 hours with 100 mg and 72 hours with 150 mg. Neither tolerance nor dependence develops with naltrexone. Oral naltrexone is approved for relapse prevention of alcohol and opioid dependence in several countries including the UK, and its use for relapse prevention dates back to the 1960s. In general, clinical research on naltrexone over the past few decades indicates that it is safe, associated with few side effects, and clearly blocks the reinforcing properties of heroin and other opiates. Nonetheless its use remains limited. There are probably two main reasons for this in the UK. First, it can only be used if the patient is completely clean, and only a minority of addiction treatment patients (mainly in residential settings) are detoxed to full abstinence during their initial treatment. Second, naltrexone is only licenced for use in oral (tablet) form and there is an all too frequent tendency for the recovering patient to be triggered into skipping the naltrexone tablets and relapsing to the original patientive substance. Once this has happened it is difficult to get back to the naltrexone course without another detox. The solution to the poor adherence experienced with oral naltrexone is to move to sustained release formulae such as implants or injections.
Naltrexone does also add to the cost of the treatment which may be another constraint.
In addition to its use specifically for relapse prevention treatment, naltrexone is also one of the non patientive drugs commonly used in medication assisted detoxes, along with lofexidine or clonidine.
3. Which Drugs are most effective at preventing relapse?
Naltrexone is the only effective relapse prevention drug. The most common tablet forms run the risk of the patient not persevering with the treatment. Slow release implants or injections offer a solution.
A constraint to the wider use of implants is that Russia is currently the only country in the world to have a licensed implant. This does not mean that naltrexone implants (or indeed injections) cannot be used outside Russia. They can be used an “unlicensed” status which means each must be on a “named patient basis”. It is expected that naltrexone will eventually secure FDA and thereafter NICE approval.
The injectable form of Naltrexone is Vivitrol. Its use is still in the early stages.
4. Which Drugs are most effective at treating relapse?
There is no simple medication based solution to treating relapse. Relapses take many forms from incidental one-offs (that may be treated with therapies) to a full return to the original addiction implying readmission to the previous treatment. Multiple re-admissions are common in opioid recovery.
If the original or relapsed abuse leads to overdose, naloxone (not to be confused with naltrexone) is used rapidly to reverse opioid overdoses.
5. What is the New Life Centre Approach?
Acceptance of naltrexone based relapse prevention is optional for NLC patients but is highly recommended by the BONDS team given the high rates of relapse after addiction treatment, especially for opioids. Patients are required to take “challenge” test to ensure they are fully clear of any patientive substance before the naltrexone treatment can be initiated.
NLC generally favours slow release solutions. Worldwide NLC and the three other enterprises (Cameron in the USA, O’Neil in Western Australia and Heroin Detox Facility Srbija in Serbia) that have led the development of less protracted detoxes (7-14 DAY DETOX) under light sedation semi wakeful sedation . These are also the enterprises have gone furthest in developing the use of naltrexone implants. Indeed O’Neil in Western Australia has developed and 7-14 day detox the O’Neil Long Acting Implant (OLANI). This is the naltrexone implant of choice that NLC offers, and indeed NLC benefits from a long collaborative association with Dr George O’Neil. Naltrexone implants have been used in previous iterations of the BONDS treatment programmes since 2006 (when provided by Detox5 in the past). The NLC medical director has overseen the use of around 3,000 implants at Detox5 in previous years, prior to the opening of The New Life Centre at Broughton Hall. Whilst other services may market the same implants as lasting longer for example, The New Life Centre believes in safety first, and recommends that a ‘double’ OLANI should be considered as standard and it is envisaged to last on average around 6 months.
The injectable form of Naltrexone is Vivitrol. Its use is still in the early stages but NLC is viewing it as a potential preferred relapse prevention treatment for alcohol.